Unemployed Growth and the Emerging Inequality of Longevity

His recent work examines the broader socioeconomic consequences of artificial intelligence, including labor markets, public finance, demographic change, institutional adaptation, and the distributional effects of technological progress.
He holds a PhD in Mathematical Finance from Boston University, and previously earned an MSc in Finance and Economics from the London School of Economics. He completed his undergraduate studies in Economics at Seoul National University under the Korea Foundation for Advanced Studies scholarship program.
Authored on
Modified
AI can accelerate biological research, diagnosis, prevention and care, raising the prospect of longer and healthier lives Its nearer-term labour effect may be unequal augmentation: a small group becomes dramatically more productive while others lose bargaining power or move into lower-quality work Because work, income, wealth and access shape health, AI could widen longevity inequality unless its productivity and medical dividends are deliberately shared

At the Fondazione Giorgio Cini conference in Venice, I argued that artificial intelligence should be understood not only as a medical technology or a productivity technology, but also as a distributional technology. AI may push outward the frontier of healthy ageing through faster scientific discovery, earlier diagnosis and more personalised care. At the same time, it may weaken the employment, income and social-insurance foundations that allow ordinary people to benefit from medical progress. These two changes can occur together. A society may become more capable of extending life while becoming less equal in the resources required to live well. The central question, therefore, is not simply whether AI will add years to life. It is whether institutions can convert AI-driven progress into broadly shared healthspan rather than a new longevity divide.
AI may push outward the frontier of healthy ageing
The optimistic case is real and should not be understated. AI is already changing the research infrastructure of biology and medicine. Systems such as AlphaFold have made more than 200 million predicted protein structures openly available, giving scientists a faster starting point for understanding biological mechanisms and developing treatments.[1] AI is also being used to identify molecular targets, model interactions, analyse medical images, predict clinical risk and support earlier intervention. The United States Food and Drug Administration now maintains a public list of AI-enabled medical devices that have passed applicable premarket requirements, showing that AI is moving from the laboratory into regulated clinical practice.[2] In ageing research, the long-term promise is not simply more years of life, but more years without frailty, disability or chronic disease. AI could help medicine shift from late treatment toward earlier prediction and prevention. I did not argue in Venice that AI has “solved” ageing; much of the most ambitious work remains early-stage. The important point is that AI is enlarging the technical possibility set. It can accelerate discovery and improve the precision with which healthcare systems identify, monitor and treat risk.
The nearer-term labour shock may be unequal augmentation
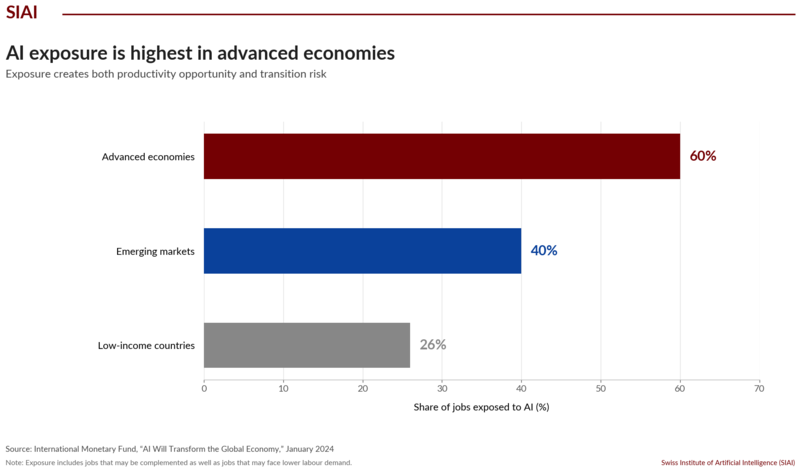
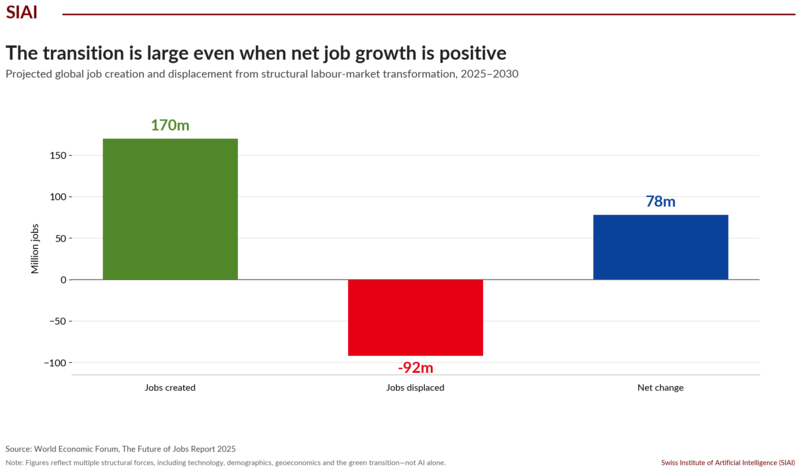
When people hear “AI and jobs,” they often imagine a distant world of robots, self-driving systems and full automation. I focused instead on the intermediate phase, because it may arrive earlier and matter more for inequality. In this phase, a relatively small group of highly AI-proficient workers becomes far more productive. They manage AI agents, compress research and analysis cycles, and scale their output without a matching increase in headcount. Other workers are not necessarily dismissed immediately, but they may lose bargaining power, see entry-level pathways narrow, or move into lower-quality work. The IMF estimates that about 60 per cent of jobs in advanced economies are exposed to AI, with some workers benefiting from complementarity and others facing lower labour demand, wages or hiring.[3] The ILO reaches a more cautious but compatible conclusion: one in four workers globally is in an occupation with some generative-AI exposure, while job transformation is more likely than wholesale replacement.[4] The World Economic Forum projects 170 million jobs created and 92 million displaced by 2030.[5] A positive net number does not guarantee a benign transition. The new jobs may appear in different places, require different skills and arrive too late for the people whose careers are disrupted.
Why labour inequality becomes longevity inequality
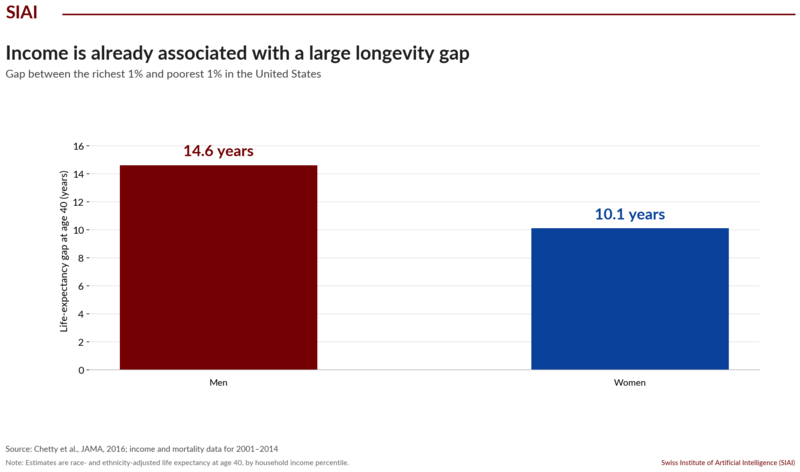
This labour-market transition matters for longevity because health is not produced by medicine alone. It is produced over a lifetime through income, housing, education, nutrition, working conditions, autonomy, stress, neighbourhood quality, social support, healthcare access and retirement security. The World Health Organization describes these as the conditions in which people are born, grow, work, live and age, and notes that health follows a social gradient: lower income and greater deprivation are associated with worse health and fewer healthy years.[6] Existing evidence shows how large the gap can become. A major US study using 1.4 billion person-year observations found that, at age 40, the richest 1 per cent lived 14.6 years longer than the poorest 1 per cent among men and 10.1 years longer among women.[7] AI does not create this relationship from nothing. It enters a world in which lifetime income and wealth already shape longevity. If AI concentrates productivity gains among capital owners and highly adaptable workers while weakening wages, career stability and pension accumulation for others, it can become an indirect driver of health inequality. A labour-market shock can therefore become a healthspan shock, even when the technology is simultaneously improving clinical capability.
The emerging longevity divide is also an access and data divide
The resulting divide will not be defined only by who can afford a future anti-ageing therapy. It will also depend on who can use the full ecosystem of AI-enabled prevention. One group may have stable income, strong insurance, digital literacy, high-quality health records, wearable data, regular screening and access to clinicians who can interpret algorithmic recommendations. Another group may face unstable employment, fragmented records, limited digital access, delayed care and little ability to act on an early warning even when one is available. Data representation creates a further layer of inequality. If models are trained mainly on populations that are wealthy, insured, urban and digitally visible, performance may be weaker for people who are underrepresented or medically underserved. AI systems may also become gatekeepers: deciding who receives additional screening, priority, referral or follow-up. The emerging “AI-augmented longevity class” will therefore be defined by more than income. It will include people who are legible to data systems, capable of navigating digital care and able to convert prediction into action. Others may receive the promise of personalised medicine without the institutional capacity to benefit from it.
The executive agenda is to distribute both dividends
For executives, policymakers and educators, the practical message is that AI strategy needs a wider scorecard. It is no longer enough to ask how much cost can be removed, how many tasks can be automated or how rapidly output can scale. Leaders should also ask who is being augmented, who is being displaced, how quickly roles are changing, whether entry-level career ladders remain viable, and how productivity gains are shared through wages, training, benefits and retirement security. Training is essential, but it is not a complete answer: some workers need time, mobility support, redesigned jobs and credible pathways into new roles, not simply another online course. In healthcare, leaders should treat AI-enabled diagnosis and prevention as potential public infrastructure rather than solely as premium services. Models should be evaluated across age, income, geography and demographic groups, while data governance should make underserved populations more visible without weakening privacy. My closing point in Venice was that AI will shape longevity twice: first through biology, and second through the social structure of work and income. The aim should be to ensure that AI-driven growth becomes AI-shared healthspan. Otherwise, we may solve parts of biological ageing faster than we solve the inequality that determines who benefits.
Selected sources
1. AlphaFold Protein Structure Database, EMBL-EBI and Google DeepMind.
2. Artificial Intelligence-Enabled Medical Devices, U.S. Food and Drug Administration.
5. World Economic Forum, The Future of Jobs Report 2025, 7 January 2025.
6. World Health Organization, “Social Determinants of Health”.
His recent work examines the broader socioeconomic consequences of artificial intelligence, including labor markets, public finance, demographic change, institutional adaptation, and the distributional effects of technological progress.
He holds a PhD in Mathematical Finance from Boston University, and previously earned an MSc in Finance and Economics from the London School of Economics. He completed his undergraduate studies in Economics at Seoul National University under the Korea Foundation for Advanced Studies scholarship program.